Obamacare:
Assessing the Legacy of President Obama through his Flagship Legislation...
...And What the Republicans
Need to Do to Fix It
In March 2010, Barack Obama signed into law the Affordable Care Act, otherwise known as "Obamacare". A year later, the Supreme Court defended and approved the Federal Government's right to enact this legislation, citing its powers of taxation of revenue.
William Galston, a key political adviser in the Clinton Administration, is quoted as saying, "The A.C.A. (Obamacare) is the signature achievement of his Administration and one of the biggest promissory notes ever handed to the American people. It's not only his moral obligation to deliver on this promise, but an absolute political necessity."
But, as the years went on, Obamacare's problems started to surface, so much so that president-elect Donald Trump vowed to "repeal and replace Obamacare with something terrific" if he were to be elected. Why does he want to replace it? And with what system? Before we answer that, we need to understand, first:
Using your provided sheet, answer the questions below.
William Galston, a key political adviser in the Clinton Administration, is quoted as saying, "The A.C.A. (Obamacare) is the signature achievement of his Administration and one of the biggest promissory notes ever handed to the American people. It's not only his moral obligation to deliver on this promise, but an absolute political necessity."
But, as the years went on, Obamacare's problems started to surface, so much so that president-elect Donald Trump vowed to "repeal and replace Obamacare with something terrific" if he were to be elected. Why does he want to replace it? And with what system? Before we answer that, we need to understand, first:
- What is wrong with America's healthcare, and
- What Obamacare aimed to accomplish in the first place.
Using your provided sheet, answer the questions below.
Part I:
The "Need"
for Obamacare
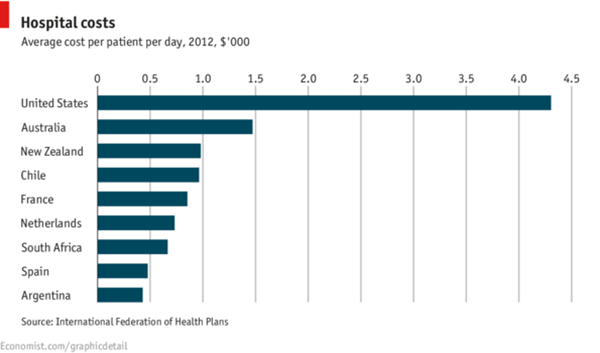
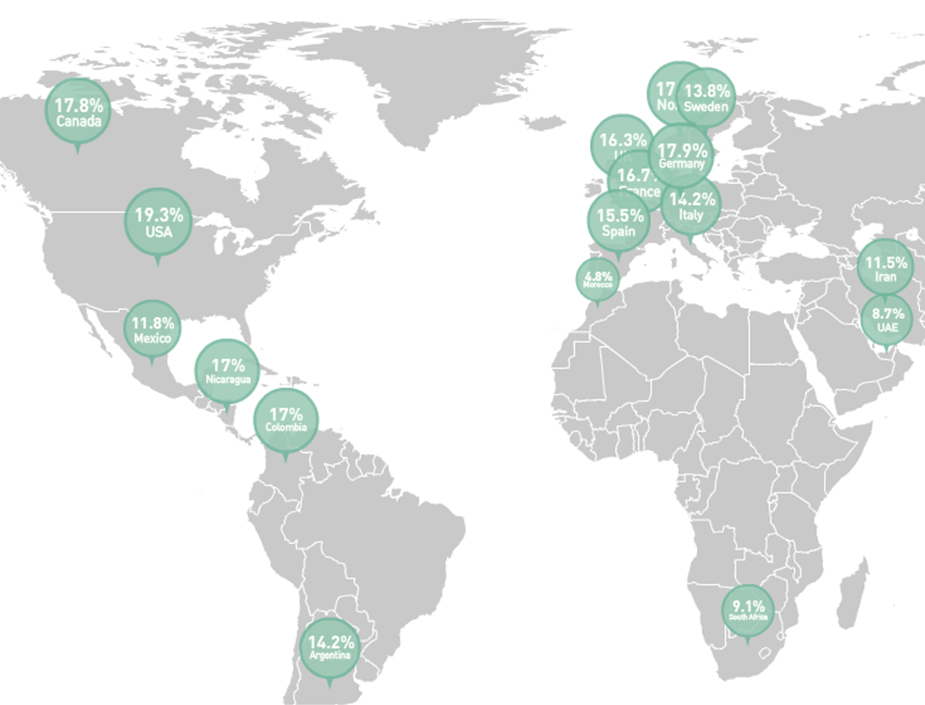 Health Care Expenditure as a % of GDP.
Health Care Expenditure as a % of GDP.
As compared with other nations, the United States spends the most money on health care, but has fewer doctors and shorter life expectancies.
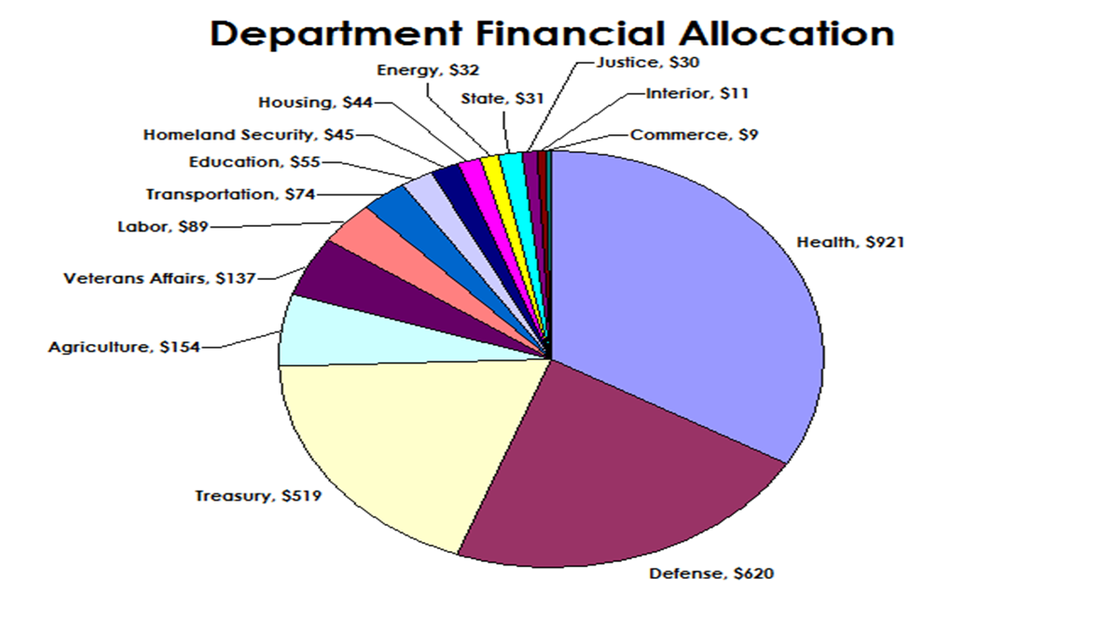 Annual governmental expenditure based on financial allocation to each federal department.
Annual governmental expenditure based on financial allocation to each federal department.
Additionally, the spending on health care totals close to by over $1 trillion and exhibits no sign of slowing down.
So...there's a problem here: The government spends more money, but we have fewer doctors and shorter life expectancies. Additionally, if the government is spending all this money, when then is health care so darn expensive?
TIME Magazine covered this very issue in March 2013. The title of the featured article was called "The Bitter Pill: Why Medical Bills are Killing Us" and explores the problems with the current health care system. To be able to understand the need for Obamacare, we must start by understanding why health care was broken in the first place.
Read excerpts from the article below and answer the accompanying questions.
TIME Magazine covered this very issue in March 2013. The title of the featured article was called "The Bitter Pill: Why Medical Bills are Killing Us" and explores the problems with the current health care system. To be able to understand the need for Obamacare, we must start by understanding why health care was broken in the first place.
Read excerpts from the article below and answer the accompanying questions.
1: The "Basic Problems"
The article starts out by discussing some of the "basic problems" with today's health care system. And it discusses "cost" first. Read the excerpts below:
- In the U.S., people spend almost 20% of the gross domestic product (the country's "worth") on health care, compared with about half that in most developed countries. Yet in every measurable way, the results our health care system produces are no better and often worse than the outcomes in those countries… We spend more on health care than the next 10 biggest spenders combined: Japan, Germany, France, China, the U.K., Italy, Canada, Brazil, Spain and Australia.
- According to the Center for Responsive Politics, the pharmaceutical and health care product industries, combined with organizations representing doctors, hospitals, nursing homes, health services and other health insurance programs, have spent $5.36 billion since 1998 on lobbying in Washington. That dwarfs the $1.53 billion spent by the defense and aerospace industries and the $1.3 billion spent by oil and gas interests over the same period. That’s right: the health care industrial complex spends more than three times what the military industrial complex spends in Washington.
- Of the total $2.8 trillion that will be spent on health care, about $800 billion will be paid by the federal government through the Medicare insurance program for the disabled and those 65 and older and the Medicaid program, which provides care for the poor. That $800 billion, which keeps rising far faster than inflation and the gross domestic product, is what’s driving the federal deficit. The other $2 trillion will be paid mostly by private health insurance companies and individuals who have no insurance or who will pay some portion of the bills covered by their insurance.
- In the U.S., people spend almost 20% of the gross domestic product (the country's "worth") on health care, compared with about half that in most developed countries. Yet in every measurable way, the results our health care system produces are no better and often worse than the outcomes in those countries… We spend more on health care than the next 10 biggest spenders combined: Japan, Germany, France, China, the U.K., Italy, Canada, Brazil, Spain and Australia.
1. If you've ever wanted to know about the basic problems with today's health care, it's right here, and it starts with "cost". Describe three (3) problems with today's health care in terms of "cost".
The article continues to discuss the "basic problems" with today's health care system by defining the "victims" inside of the system. Read the excerpts below:
- People fare differently according to circumstances they can neither control nor predict. They may have no insurance. They may have insurance, but their employer chooses their insurance plan and it may limit how much they employer will pay or which drugs and treatment they'll cover. They may or may not be old enough to be on Medicare (a health care program for senior citizens) or be poor enough to be on Medicaid, the government-assisted program that provides for low-cost health care…And if you're not protected by Medicare, the health care market is not a market at all. It’s a crapshoot…
- Additionally, most Americans today have little visibility into pricing, let alone control of it. And if they do have access to the bill, they have no idea what the bill means. They have little choice of hospitals or the services they are billed for, even if they somehow know the prices before they get billed for the services.
- They have no choice of the drugs that they have to buy or the lab tests or body scans that they have to get, and they would not know what to do if they did have a choice.
- They are powerless buyers in a seller’s market where the only sure thing is the profit of the sellers. Since 2011, there have been more than 3.5 million personal bankruptcies filed in the U.S. Some 60%, or more than 2 million, are estimated to have involved medical debt as a key factor.
2. Continue to define the "problems" by identifying why and how people are being "victimized".
2: The Government Bureaucracy
In the 1930s, Franklin Roosevelt created the Social Security Administration to help those in need of government support through unemployment relief, retirement savings, and basic health care services. During World War II, the federal government "froze" the profits of private businesses, but allowed these same businesses to attract and retain employees by offering certain "benefits", such as health insurance. In the 1960s, Lyndon Johnson created the Medicare system (which later expanded into Medicaid in the 1980s) to help the elderly and the poor pay for health care. And today, we find that not much has changed. Read the excerpts below:
- Medicaid covers more people: 56.2 million compared with 50.2 million with Medicare.
- More than 3 million bills that come into Medicare every day. The system then figures out the right payments for each person and churns out more than $1.5 billion a day in wire transfers.
- However, hospital finance people argue vehemently that Medicare doesn’t pay enough and that they lose as much as 10% on an average Medicare patient.
- Medicare spent more than $6.5 billion last year to pay doctors, but these payments are at a deeply discounted Medicare rates. Remember that Medicare / Medicaid is for the elderly and the poor, so "cost" to the patients is very low. The difference between what the patient pays and what the doctors charge is paid by the federal government. Depending on the discount, a Medicare patient can pay anywhere from $7.48 to $164 for a chest X-Ray reading.
- One such patient we interviewed had 33 visits in one year to 11 doctors who had nothing to do with his recovery from the heart attack or his cancer. In all cases, he was routinely asked to pay almost nothing: $2.20 for a check of a sinus problem, $1.70 for an eye exam, 33¢ to deal with a bunion. “They paraded in once a day or once every other day, looked at me and poked around a bit and left,” Alan A. recalls. Other than the doctor in charge of his heart attack recovery, “I had no idea who they were until I got these bills. But for a dollar or two, so what?”
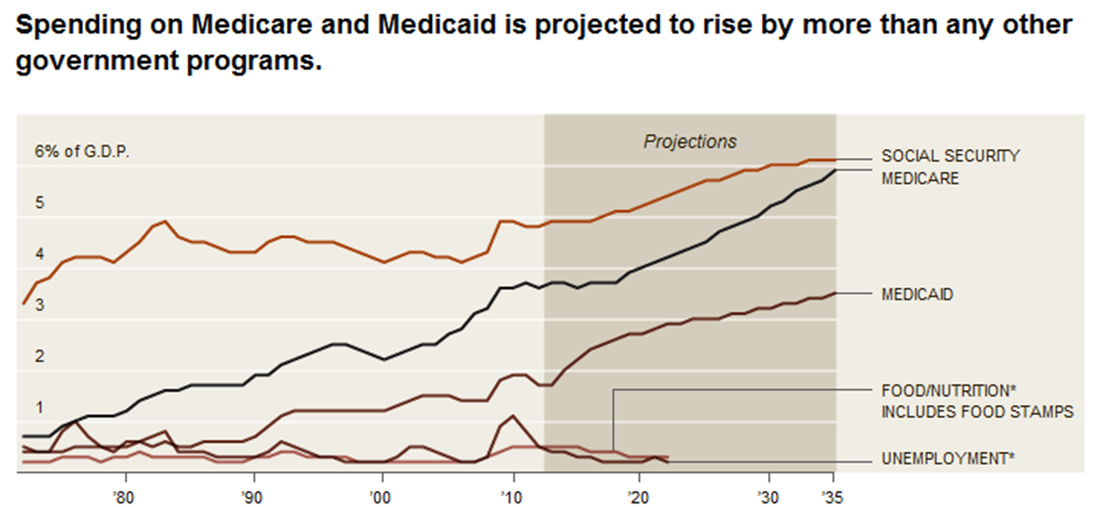
Government expenditures as a % of GDP.
3. If you add it up, the federal government spends $800 billion per year to cover approximately 90 million people (1/3 of our country's population). That's a lot of people and a lot of money! But that's not the issue. What's one thing you've learned about Medicare / Medicaid that's "problematic"?
3. The "Cost"
So far, we've learned that the United States allocates approximately 20% of its budget to health care. We've also learned that Medicare / Medicaid covers about 90 million people and costs $800 billion per year. So, with all this spend, why are medical bills so high? That's what this article set out to answer. Let's start with the graphic below.
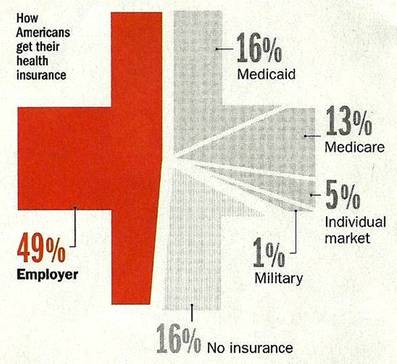
Most Americans get their health care from their "employer", meaning that their employer "pays" most of their monthly bill, or "subscription" to health care, and just charges the employee a smaller fee. This "smaller fee" can vary: A public school teacher, for example, might pay $15 per month for health care while their school district picks up the rest of the bill. Conversely, a businessman in a private business (Starbucks, for example...) might pay $200 to $300 per month. It all depends.
4. Fill in the blanks, using the percentages above: There are about 300 million people in America today. About _____ million have "employer-sponsored" health care; _____ million people rely on Medicare / Medicaid for their insurance, and about _____ million "buy" their insurance on the "individual market", just as you would buy a Comcast subscription for TV and internet. And there are about _____ million Americans who are completely uninsured.
Let's continue to read excerpts from the article and try to answer why health care is so expensive.
4. Fill in the blanks, using the percentages above: There are about 300 million people in America today. About _____ million have "employer-sponsored" health care; _____ million people rely on Medicare / Medicaid for their insurance, and about _____ million "buy" their insurance on the "individual market", just as you would buy a Comcast subscription for TV and internet. And there are about _____ million Americans who are completely uninsured.
Let's continue to read excerpts from the article and try to answer why health care is so expensive.
- When Sean Recchi, a 42 year old from Lancaster, Ohio, was told last March that he had non-Hodgkin’s lymphoma, his wife Stephanie knew she had to get him to MD Anderson Cancer Center in Houston, Texas. Stephanie was then told by a billing clerk that the estimated cost of Sean’s visit — just to be examined for six days so a treatment plan could be devised — would be $48,900, due in advance. The total cost for Sean to get his treatment plan and initial doses of chemotherapy was $83,900.
- Soon after he was diagnosed with lung cancer in January 2011, a patient whom I will call Steven D. and his wife Alice knew that they were only buying time. The crushing question was, How much is time really worth? Alice had collected bills totaling $902,452. They had maxed out on the $50,000 payout limit on a UnitedHealthcare policy they had bought through a community college where Steven had briefly enrolled a year before. A "payout limit" is the maximum amount of money that a health insurance company will pay. After that, the bills are up to you! “We were in shock,” Alice recalls. “We looked at the total and couldn't deal with it. So we just started putting all the bills in a box. We couldn't bear to look at them."
- There was no way the D.’s or Sean Recchi could pay those bills...so what happens?
- Consider another case involving a 61-year-old bus driver named Emilia Gilbert who slipped and fell one evening in her backyard in Fairfield, Connecticut. She was taken to the emergency room at Bridgeport Hospital, where she was treated for some cuts and a broken nose. She left a few hours later with a bill for $9,418, which included $6,538 for CT scans and $239 for a routine blood test. When Gilbert, who was earning about $22,000 a year, was unable to pay, she was sued by the hospital. A judge ordered her to pay off her bill in $20 weekly payments over six years.
- That's one solution: long payment plans. The D.'s were able to scrape together $3,000. With the couple’s $3,000, on top of the $50,000 paid by the UnitedHealthcare insurance, that leaves a bill of almost $850,000. Hospitals can put the D.'s or the Recchi's on a payment plan, but these plans would take hundreds of years to pay off! So hospitals just "write it off" in the form of "discounts"....
- What is a "write off"? Let's look at the numbers: Of the $900,000 bill the hospital charged, they only received $53,000. Technically, that's the only revenue (profit) they collected. When it comes time to pay taxes to the government, they only pay taxes on the $53,000, completely ignoring the $850,000 debt because it's "written off"....
- The government is now "missing out" on its tax money. "Write offs" are legal and normal, as the government allows them. BUT! They government is STILL NOT GETTING the taxes they're due! And that's part of the reason why we have such a high debt today...
- According to a recent financial report, some hospitals apply so many discounts and write-offs that they end up with only about 18% of the revenue it bills for. That’s an average 82% discount.
- When the discounts to Medicare and private insurers are applied, hospitals end up being paid a lot less overall than what is itemized on the original bills. One particular hospital studied ended up receiving about 35% of what it bills to patients. This money is left unpaid...and that's that...
5. ...but that's NOT that! We'll deal with it later, but for now, summarize the problems that surround the cases of the D.'s and the Recchi's.
6. So...what is a "write off"? What does it to do the government? (NOTE: ...and if you're smart, can you see how this "indirectly" leads to higher medical prices? Because the bills aren't gettin' paid!)
Let's continue on...
7. What is a "chargemaster"? Why is it "problematic"?
8. These charges for alcohol prep pads, diabetes testing strips, and others...aside from the price of a CT scan...are just ridiculously high. ANALYSIS: Can you predict why?
Are there other reasons why medical bills are so high? The answer....YES!
6. So...what is a "write off"? What does it to do the government? (NOTE: ...and if you're smart, can you see how this "indirectly" leads to higher medical prices? Because the bills aren't gettin' paid!)
Let's continue on...
- Why exactly are the bills so high? For one, it has to do with something called a "chargemaster". The chargemaster, I learned, is every hospital’s internal price list. Decades ago it was a document the size of a phone book; now it’s a massive computer file, thousands of items long, maintained by every hospital.
- No hospital’s chargemaster prices are consistent with those of any other hospital, nor do they seem to be based on anything objective — like cost — that any hospital executive I spoke with was able to explain. “They were set in cement a long time ago and just keep going up almost automatically,” says one hospital chief financial officer with a shrug… An “NM MYO REST/SPEC EJCT MOT MUL” was billed at $7,997.54. That’s a stress test using a radioactive dye that is tracked by an X-Ray computed tomography, or CT, scan. That's a very high cost for a "CT Scan". Additionally, another problem is that Medicare only pays the hospital about $550 for that test.
- Dozens of mid-priced items were embedded with similarly aggressive markups, like $283.00 for a “CHEST, PA AND LAT 71020.” That’s a simple chest X-Ray for which one hospital is routinely paid $20.44 when it treats a patient on Medicare. Here are additional "bills" that we found alarming:
- Sean Recchi’s single dose of Rituxan, a drug to combat his aggressive cancer, costs as little as $300 to make, test, package and ship to to the hospital. They charge the hospitals $3,000 to $3,500, whereupon the hospital sold it to Recchi for $13,702.
- The charge to have a doctor simply read a CT scan? $261.00
- The price for one “ALCOHOL PREP PAD": $7.00. This is a little square of cotton used to apply alcohol to an injection. A box of 200 can be bought online for $1.91.
- "Niacin" is a drug used to lower cholesterol. A charge for (1) niacin pin? $24.00
- The charge for (1) diabetes test strip? $18.00
- And yes...there was a bill for attaching a shade to an examining lamp...
7. What is a "chargemaster"? Why is it "problematic"?
8. These charges for alcohol prep pads, diabetes testing strips, and others...aside from the price of a CT scan...are just ridiculously high. ANALYSIS: Can you predict why?
Are there other reasons why medical bills are so high? The answer....YES!
4. Tests, Tests, and More Tests...
By now, we've seen that Medicare / Medicaid covers about 90 million people, and that one of the biggest problems is that hospitals don't get PAID enough in return! Hospitals run a deficit and this deficit is passed on to the federal government. Perhaps that's why they charge so much for tests, testing strips, and alcohol pads. Another problem we see is that, quite frankly, Americans have TOO MUCH health care! Read below:
9. It seems like one of America's biggest problems is the number of "tests" we require. But it might not be the doctors' fault! Why do doctors use so many tests?
- A recent report found that health care providers in the U.S. conduct far more CT tests per person than those in any other country — 71% more than in Germany, for example, where the government-run health care system offers none of those incentives for over-testing. We also pay a lot more for each test, even when it’s Medicare doing the paying.
- According to a study in the Annals of Emergency Medicine, the use of CT scans in America’s emergency rooms “has more than quadrupled in recent decades.” As one former emergency-room doctor puts it, “Giving out CT scans like candy in the ER is the equivalent of putting a 90 year-old grandmother through a pat-down at the airport: Hey, you never know.”
- “We use the CT scan because it’s a great defense,” says the CEO of another hospital not far from Stamford. “For example, if anyone has fallen or done anything around their head — hell, if they even say the word head — we do it to be safe. We can’t be sued for doing too much.” This is to defend against medical malpractice litigation, in other words, people "suing" the doctors because of something they did wrong.
- Said one doctor, “I bet 60% of the labs are not necessary.” Said another, “They
hand out blood tests and Xrays in hospitals like bottled water, and they know
it.”
9. It seems like one of America's biggest problems is the number of "tests" we require. But it might not be the doctors' fault! Why do doctors use so many tests?
5. Follow the Money...
Trillions spent. Billions in write-offs. Thousands of dollars in medical bills. Someone must be profiting off this, right? Read below:
Now, this article is NOT arguing that doctors and hospitals should not be paid, nor should they collect as much money as possible! After all, they do save lives! And also, remember that so many prices are "inflated" to cover the "write-offs" and "discounts" they offer. BUT! Let's record some data and answer some questions.
10. What was MD Anderson's profit? Stamford's?
11. "Profits" can be cyclical. If a hospital makes significant profit, what then do they do with that money? And in turn, how does this make MORE profit?
12. How do medical devices and machines make doctors profits as well?
- MD Anderson, a hospital in Austin, Texas, and the same one who treated Sean Recchi's cancer, has a profit that exceeds $531 million per year. That’s a profit margin of 26% on revenue of $2.05 billion, an astounding result for such a service-intensive enterprise.
- Stamford Hospital, the same one who treated the D's, managed an operating profit of $63 million on revenue actually received, even after all the discounts off the chargemaster prices. That’s a 12.7% operating profit margin, which would be the envy of shareholders of high-service businesses across other sectors of the economy
- As hospitals improve and expand facilities, they buy more equipment, hire more people, offer more services, buy rival hospitals and then raise executive salaries because their operations have gotten so much larger. They keep the upward spiral going by marketing for more patients, raising prices and pushing harder to collect bill payments.
- In 2008, Gregory Demske, an assistant inspector general at the Department of Health and Human Services, told a Senate committee that “doctors routinely receive substantial compensation [payment] from medical-device companies through stock options, royalty agreements, consulting agreements, research grants and fellowships.” In other words, if doctors "buy their products", they get paid handsomely.
- According to a McKinsey study of the medical marketplace, a typical piece of equipment will pay for itself in one year if it carries out just 10 to 15 procedures a day. That’s a terrific return on capital equipment that has an expected life span of seven to 10 years. And it means that after a year, every scan ordered by a doctor in the Stamford Hospital emergency room would mean pure profit, less maintenance costs, for the hospital.
- Overall prescription drug prices in the U.S. are “50% higher for comparable products” than in other developed countries. [Remember Sean Recchi's cancer treatment cost $300 to make, was sold to the hospitals for $3,000, and was "sold" to Sean for over $13,000...]
Now, this article is NOT arguing that doctors and hospitals should not be paid, nor should they collect as much money as possible! After all, they do save lives! And also, remember that so many prices are "inflated" to cover the "write-offs" and "discounts" they offer. BUT! Let's record some data and answer some questions.
10. What was MD Anderson's profit? Stamford's?
11. "Profits" can be cyclical. If a hospital makes significant profit, what then do they do with that money? And in turn, how does this make MORE profit?
12. How do medical devices and machines make doctors profits as well?
Conclusion
Remember: the goal of this activity was to see what Obamacare WANTED TO FIX! Next class, we'll look at the Republican plan to fix Obamacare! But, for now: Complete the "fill-in" story on your provided sheet.
